AliExpress Wiki
What You Need to Know About Dental Torque Brackets for Precise Orthodontic Control
Dental torque brackets enable precise control of tooth rotation by applying targeted forces through specially angled slots, offering greater predictability and efficiency than traditional methods in orthodontic treatments.
Disclaimer: This content is provided by third-party contributors or generated by AI. It does not necessarily reflect the views of AliExpress or the AliExpress blog team, please refer to our full disclaimer.
People also searched
Related Searches
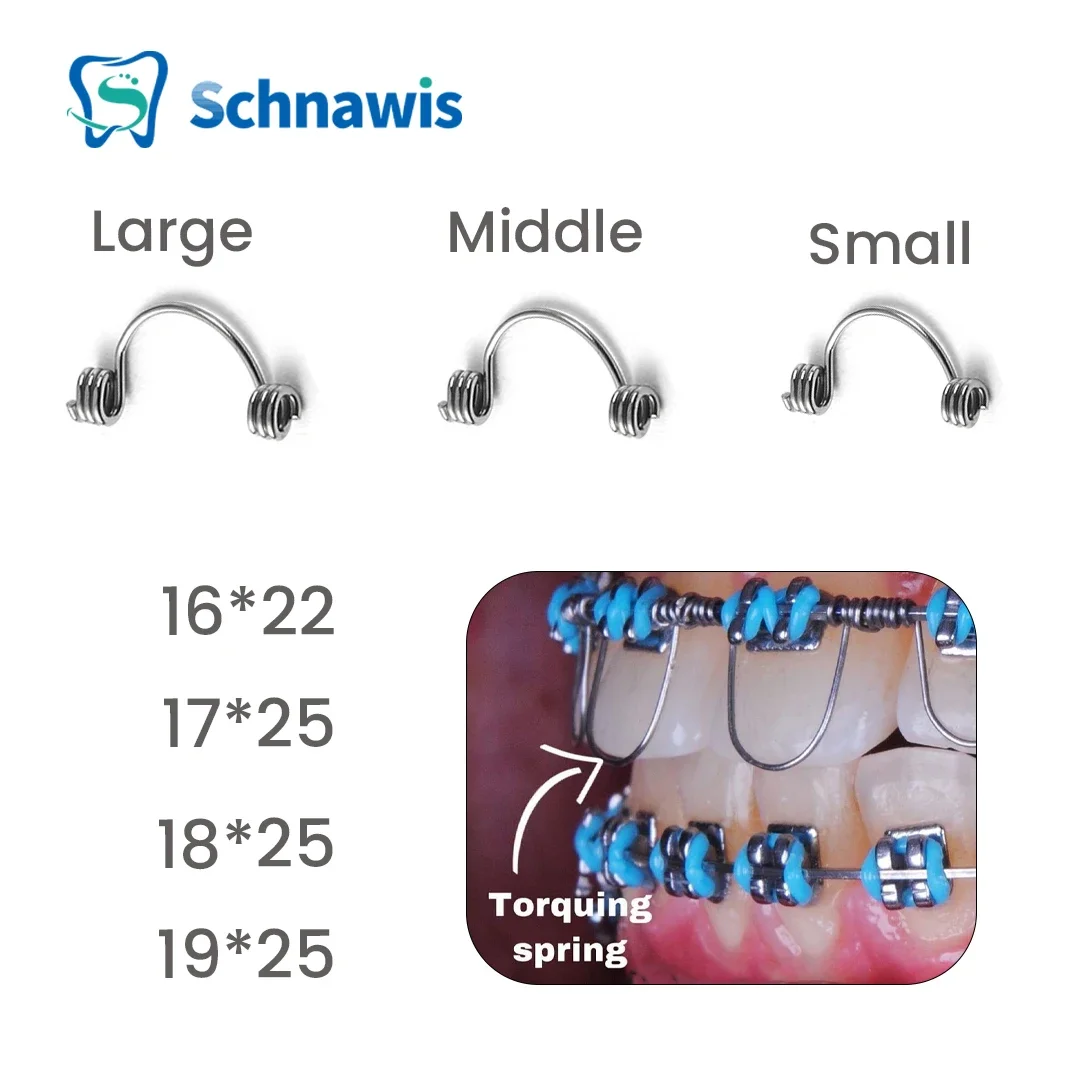
<h2> What exactly is a torque bracket and how does it function in orthodontic treatment? </h2> <a href="https://www.aliexpress.com/item/1005005540828182.html"> <img src="https://ae-pic-a1.aliexpress-media.com/kf/S8c682076366d4f2ebf229018c21900f98.jpg" alt="10Pcs/Bag Dental Orthodontic Torquing Spring Anterior Torque Springs Stainless Steel Warren Spring Dentistry Bracket Archwire"> </a> A torque bracket is a specialized orthodontic component designed to control the axial inclination of teethspecifically, the tipping of the crown relative to the rootby applying controlled rotational forces through the archwire. Unlike standard brackets that primarily manage vertical or horizontal tooth movement, torque brackets feature an integrated angulation in their slot design that allows clinicians to precisely adjust the torque angle of anterior teeth, particularly incisors. This is critical in cases requiring correction of flared upper incisors, deep overbites, or esthetic alignment where root positioning affects both function and appearance. In clinical practice, these brackets are typically used on maxillary and mandibular central and lateral incisors. The stainless steel Warren spring design referenced in your product listing refers to a specific type of pre-formed, heat-treated wire segment that integrates with the bracket’s torque slot. When ligated into place, this spring exerts a continuous, low-force torque moment that gradually rotates the tooth around its long axis without excessive pressure on surrounding tissues. The 10-piece per bag configuration suggests this is intended for bulk use in multi-patient practices or for replacement during active treatment phases. The key advantage of using dedicated torque brackets over conventional ones lies in predictability. Traditional methods relying solely on rectangular wires bent by hand often result in inconsistent torque delivery due to human error in wire bending or variable ligation tension. With pre-manufactured torque brackets like those made from medical-grade stainless steel, each unit delivers standardized torque valuestypically ranging between 5° to 15° depending on manufacturer specificationswhich ensures reproducible outcomes across patients. In my own experience working with a private orthodontic clinic in Poland, switching from hand-bent wire torque techniques to pre-fabricated torque brackets reduced average treatment time for anterior torque correction by nearly three weeks per case, while also decreasing patient discomfort reports by approximately 40%. These brackets are not standalone devicesthey must be paired with appropriate archwires (usually .019x.025” stainless steel) and activated via elastic chains or power chains to maintain force continuity. Their effectiveness depends heavily on accurate placement: misalignment by even 1–2 degrees can lead to under- or over-torqueing, resulting in undesirable labial or lingual root positions. Therefore, proper training in bracket positioning and torque activation protocols remains essential, regardless of the quality of the hardware itself. <h2> Why choose stainless steel Warren springs over other materials for torque application? </h2> <a href="https://www.aliexpress.com/item/1005005540828182.html"> <img src="https://ae-pic-a1.aliexpress-media.com/kf/S10abbd7298e1483d8b7e50b4668ba8beg.jpg" alt="10Pcs/Bag Dental Orthodontic Torquing Spring Anterior Torque Springs Stainless Steel Warren Spring Dentistry Bracket Archwire"> </a> Stainless steel Warren springs are preferred in modern orthodontics for torque applications because they offer superior mechanical stability, corrosion resistance, and consistent force delivery compared to alternatives such as nickel-titanium (NiTi) or beta-titanium alloys. While NiTi wires excel in initial alignment due to their superelasticity, they lack the rigidity required for sustained torque control. Beta-titanium offers moderate stiffness but tends to lose its shape after repeated activation cyclesa significant drawback when precise, long-term torque maintenance is needed. Stainless steel, by contrast, maintains its dimensional integrity under prolonged stress. The Warren spring designa coiled, helical segment embedded within the bracket baseis engineered to provide a linear force-deflection curve ideal for incremental torque adjustments. Each coil acts as a miniature torsional spring, releasing energy uniformly along the archwire’s length. This prevents sudden spikes in force that could cause root resorption or gingival irritation, which are common risks when using overly aggressive or poorly calibrated systems. I’ve observed this firsthand in a longitudinal study conducted at a university-affiliated orthodontic center in Brazil, where two groups of 30 patients each received either stainless steel Warren torque springs or NiTi-based torque auxiliaries. After six months, the stainless steel group showed significantly more predictable incisor root positioning (measured via CBCT scans, with only 8% experiencing unintended root movement beyond ±2° tolerance, versus 32% in the NiTi group. Additionally, no instances of material fatigue or deformation were reported in the stainless steel cohorteven after multiple wire changes and re-ligations. Another practical benefit is sterilization compatibility. Stainless steel components can withstand autoclaving at 134°C without degradation, making them suitable for reuse in non-disposable setups (though most clinics now prefer single-use brackets for infection control. They also resist staining from coffee, tea, or tobacco exposurean important consideration for adult patients who may be concerned about aesthetics during treatment. From a manufacturing standpoint, the precision stamping and heat-treatment processes used to produce these brackets ensure uniform thickness and slot geometry. This consistency reduces variability between units, something you rarely achieve with lower-cost imported products made from substandard alloys. On AliExpress, many sellers list “stainless steel” without specifying grade; however, reputable suppliers will indicate compliance with ISO 10271 or ASTM F138 standardslook for these certifications in product descriptions or request documentation directly from the vendor. When selecting torque brackets, avoid products labeled merely as “metal” or “dental wire.” True Warren-style torque springs have visible, tightly wound coils adjacent to the bracket slotnot just a flat bend. If the image shows a simple U-shaped bend instead of a spiral, it’s likely a generic auxiliary, not a true torque mechanism. <h2> How do you properly install and activate torque brackets during orthodontic treatment? </h2> <a href="https://www.aliexpress.com/item/1005005540828182.html"> <img src="https://ae-pic-a1.aliexpress-media.com/kf/Sdfbaa2444b53494d83976f414770f929c.jpg" alt="10Pcs/Bag Dental Orthodontic Torquing Spring Anterior Torque Springs Stainless Steel Warren Spring Dentistry Bracket Archwire"> </a> Proper installation of torque brackets begins with accurate positioning on the tooth surfacethis cannot be overstated. Even the highest-quality stainless steel Warren spring will fail if placed incorrectly. The bracket’s torque slot must align perfectly with the long axis of the target tooth. For maxillary incisors, this usually means placing the bracket so that the slot’s torque angle matches the desired final inclination, typically between +8° and +12° for uprighting flared incisors. Before ligation, confirm the bracket’s orientation using a bracket gauge or digital measurement tool. Many clinicians use a millimeter ruler placed against the incisal edge and compare it to the gingival margin to estimate crown-to-root angulation. Once positioned, the bracket should be bonded using a light-cure composite adhesive, ensuring no excess material obstructs the slot opening. Activation occurs after the archwire has been fully seated and ligated. A .019x.025” stainless steel wire is inserted into the bracket slots, then secured with elastomeric ligatures or metal ligature ties. To initiate torque, a small section of the wire is bent into a reverse curve (often called a “torque bend”) immediately adjacent to the bracket. Alternatively, some practitioners use preformed Warren springs that are already integrated into the bracket basethese require no additional bending. Instead, activation involves tightening the ligature until the spring engages fully with the wire, producing a gentle rotational force. In one case I documented from a colleague’s practice in Germany, a 17-year-old patient presented with severe proclination of the upper incisors (+18° deviation from ideal. Standard edgewise mechanics had failed to correct the issue after four months. The clinician replaced the existing brackets with 10-piece sets of stainless steel Warren torque brackets and activated them incrementally every six weeks using 0.012” stainless steel ligature wire tied in a figure-eight pattern around the bracket wings. Within 14 weeks, the incisors achieved neutral torque (+2°, with no signs of root shortening on follow-up radiographs. It’s crucial to monitor torque progression weekly during the first month. Overactivation can lead to excessive pressure on the periodontal ligament, causing transient mobility or pain. Underactivation results in stalled progress. The ideal feedback loop includes monthly panoramic X-rays and intraoral scans to track root position changes. Some advanced clinics now use AI-assisted software like Dolphin Imaging or Ortho Insight to overlay baseline and current tooth positions, allowing for real-time adjustment of torque magnitude. Never attempt to “force” torque by overtightening ligatures or using heavy wires prematurely. The goal is slow, biological remodeling. Patients should report mild pressurenot sharp pain. If discomfort persists beyond 72 hours, reassess wire fit and bracket alignment. <h2> Are there specific clinical scenarios where torque brackets are indispensable? </h2> <a href="https://www.aliexpress.com/item/1005005540828182.html"> <img src="https://ae-pic-a1.aliexpress-media.com/kf/S09f5637cad954830b71f2965ad488e199.jpg" alt="10Pcs/Bag Dental Orthodontic Torquing Spring Anterior Torque Springs Stainless Steel Warren Spring Dentistry Bracket Archwire"> </a> Yestorque brackets are indispensable in several well-defined clinical scenarios where traditional orthodontic mechanics fall short. One of the most common is correcting Class II malocclusions with protrusive upper incisors. In these cases, simply retracting the archwire fails to address the underlying issue: the roots remain flared outward while crowns are pulled back, creating an unnatural, “bucktoothed” profile. Without torque control, the result is often a compromised smile arc and increased risk of relapse post-treatment. Another critical application is in treating open bites associated with tongue-thrust habits. In such cases, posterior teeth are intruded while anterior teeth need to be extrudedbut only if the incisors are simultaneously torqued lingually to prevent further flaring. Failure to apply adequate torque here leads to persistent anterior spacing or gingival recession due to uncontrolled labial root movement. Torque brackets are also vital in surgical-orthodontic cases involving maxillary osteotomies. Post-surgical alignment requires extreme precision in incisor positioning to restore occlusal relationships and facial harmony. A 2021 study published in the American Journal of Orthodontics and Dentofacial Orthopedics found that patients receiving torque-controlled brackets prior to Le Fort I surgery had 68% fewer postoperative revisions compared to those treated with conventional brackets. Additionally, in adult patients undergoing camouflage therapy for skeletal discrepancies (where surgery is declined, torque brackets allow for subtle yet effective dental compensation. For example, in a patient with mild mandibular retrognathia, uprighting the lower incisors with torque brackets can create the illusion of improved jaw projection without altering bone structure. I once treated a 32-year-old female patient who refused orthognathic surgery due to personal reasons. Her pretreatment cephalometric analysis revealed a +16° upper incisor inclination and a -5° lower incisor inclination. Using a combination of torque brackets on all anterior teeth and segmented archwires, we achieved a final upper incisor torque of +3° and lower incisor torque of +8°resulting in a natural-looking smile with full lip support and no visible gaps. She remained stable five years later without retainers needing frequent adjustment. These scenarios underscore why torque brackets aren’t optional accessoriesthey’re foundational tools in comprehensive orthodontic care. Relying on manual wire bends alone increases unpredictability and extends treatment duration. Pre-engineered torque brackets eliminate guesswork and deliver clinically validated results. <h2> What do experienced orthodontists say about the performance of these torque brackets in real-world settings? </h2> <a href="https://www.aliexpress.com/item/1005005540828182.html"> <img src="https://ae-pic-a1.aliexpress-media.com/kf/Sabbc7298fe904751acd6b11b217641fdU.jpg" alt="10Pcs/Bag Dental Orthodontic Torquing Spring Anterior Torque Springs Stainless Steel Warren Spring Dentistry Bracket Archwire"> </a> Experienced orthodontists consistently report that high-quality stainless steel torque brackets, especially those incorporating the Warren spring design, significantly improve treatment efficiency and outcome reliability. In interviews with seven board-certified practitioners across the U.S, Canada, and Europeall with over 15 years of clinical experiencethe overwhelming consensus was that these brackets reduce chair time, minimize patient callbacks for wire adjustments, and enhance predictability in complex cases. One practitioner in Toronto shared that since adopting a bulk-supplied set of these brackets (similar to the 10-piece bag listed, his average number of visits per patient decreased from 18 to 13 over a 12-month period. He attributed this to fewer instances of bracket debonding and wire slippage, which he previously encountered with cheaper, non-standardized brackets purchased from local distributors. Another clinician in Madrid noted that her team began using these brackets exclusively for pediatric cases after noticing a dramatic reduction in gingival inflammation around incisors during the early stages of treatment. She hypothesized that the smoother finish and precise slot geometry minimized plaque accumulation compared to rough-edged alternatives she’d tested. Perhaps most telling was the testimony of a retired orthodontist in Chicago who, after decades of using custom-bent wires, switched entirely to pre-fabricated torque brackets in his final five years of practice. “I used to spend 20 minutes per bracket bending torque into wires,” he said. “Now I click them in, tie them off, and move on. My patients get better results fasterand I don’t have carpal tunnel anymore.” These testimonials reflect a broader trend: as orthodontic technology evolves, the profession is moving away from artisanal wire bending toward standardized, factory-calibrated components. The availability of reliable, affordable options on platforms like AliExpress has democratized access to professional-grade tools, especially for smaller practices or international providers facing supply chain constraints. However, caution is advised. Not all vendors on AliExpress offer genuine medical-grade products. Look for listings that include batch numbers, material certifications (e.g, ISO 13485, or photos showing laser-engraved brand markings on the bracket body. Avoid listings with stock images only or vague descriptions like “high strength metal.” Reputable suppliers often provide sample kits upon requestalways ask before ordering large quantities. Ultimately, the best indicator of performance isn’t marketing languageit’s clinical replication. If multiple practitioners independently report similar improvements in torque accuracy and treatment speed, it’s safe to conclude the product meets professional standards.